Home
Contact Me
Missy DeWitt
0
Please read carefully and fill out the form below prior to your session. Click submit once finished.
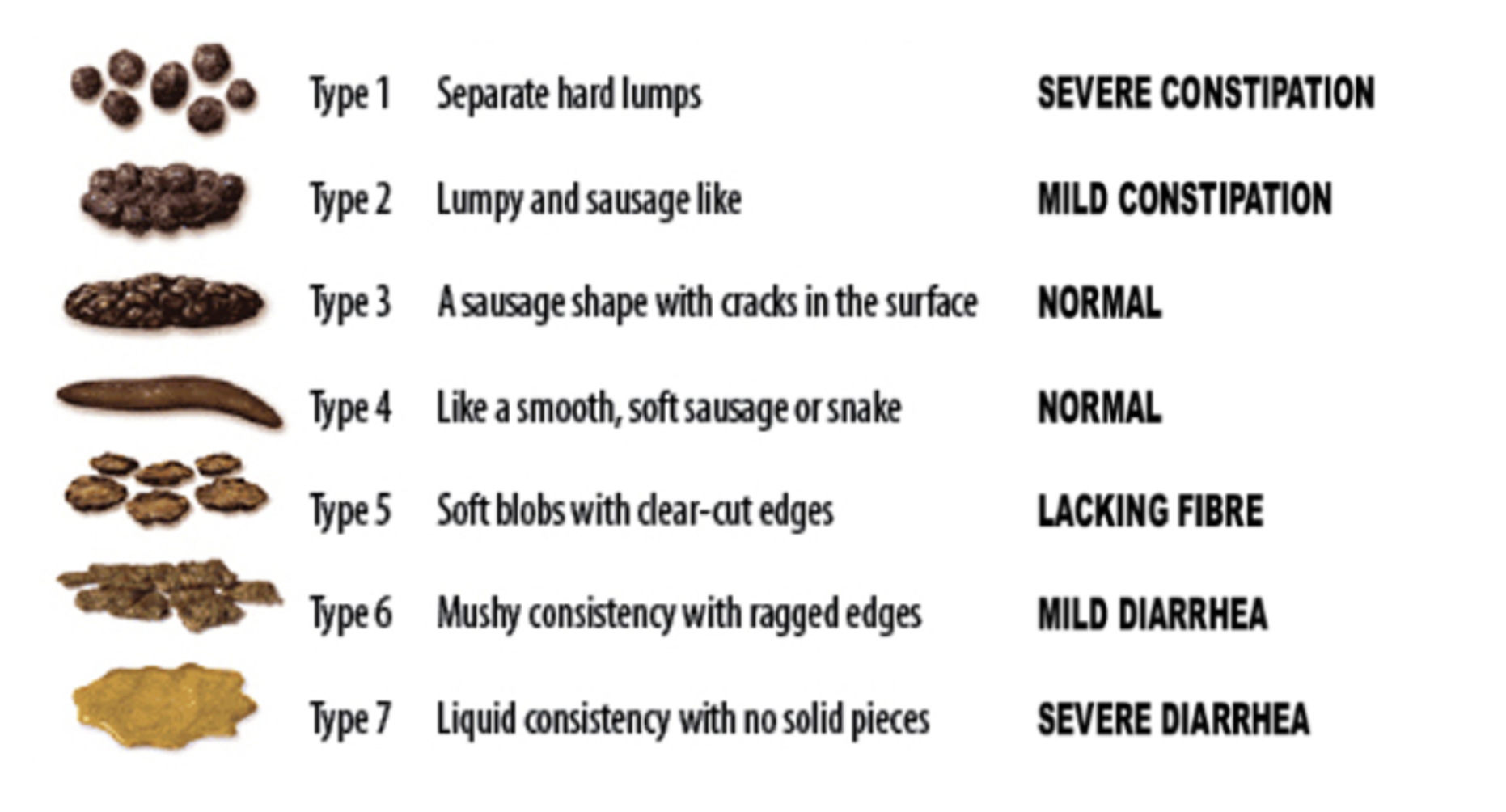
Bristol Stool Chart
0